

- Report Index
- Suicide (Jisatsu/Jishi) Prevention in Japan Part 1: Structural Challenges and the Road Ahead
- Illuminating Tomorrow
-
2025.9
Suicide (Jisatsu/Jishi) Prevention in Japan Part 1: Structural Challenges and the Road Ahead
—Reshaping Suicide (Jisatsu/Jishi) Prevention with Policy, Science, and Empathy—
Rui Shuhama
- Abstract
-
- This article constitutes Part 1 of a two-part series that examines suicide (jisatsu/jishi) in Japan from the perspectives of policy, scientific evidence, and social implementation. It provides an overview of the structural background of suicide (jisatsu/jishi) in Japan and the evolution of policy responses, with the aim of exploring effective strategies for future prevention. Part 2 of the series examines the terminology choice between jisatsu and jishi, focusing on their historical background, current usage, and implication for future suicide prevention practice.
- Suicide is shaped by multiple, overlapping risk factors-not only mental disorders, but also structural issues such as economic hardship and social isolation. Since the enactment of the Basic Act on Suicide Countermeasures (Act No. 85 of 2006; revised 2025), Japan has steadily advanced its legal framework, including explicit provisions to protect children's lives. Effective implementation requires harmonizing scientific evidence with public demand, avoiding reliance on anecdotal experience alone, and ensuring continuous evaluation and redesign of measures. Looking ahead, participatory policymaking, inclusive support for those who struggle to raise their voices and the bereaved by suicide, and a societal embrace of "responsibility grounded in empathy" are indispensable.
1. Introduction
In recent decades, the situation surrounding suicide (jisatsu/jishi) in Japan has fluctuated between improvement and deterioration. After 1998, the number of annual suicides abruptly rose to over 30,000 and remained at that high level for more than a decade. In response, a variety of policy measures were attempted, after which a temporary decline was observed. However, whether this decline can be attributed to policy interventions, natural variation, or other unknown factors remains contested. More recently, age-stratified patterns have emerged (MHLW, 2024): while increases are most striking among young women—historically a low-rate group—there has also been a renewed rise among middle-aged cohorts such as those in their 50s. These developments underscore that the situation remains highly uncertain and call for the continued evolution and refinement of suicide prevention policies.
This report reviews the trajectory of Japan's suicide-related policies and legislation, examines current challenges, and identifies directions for future countermeasures. In this report, the paired expression Suicide (jisatsu/jishi) is used. While jisatsu is the standard term in official statistics, law, and medical contexts, jishi is widely employed in bereavement support and advocacy. Usage differs depending on context and perspective, and here both terms are included together. The terminology issue will be examined in greater detail in the next report of this series.
2. Current Situation and Background Factors of Suicide (jisatsu/jishi)
Suicide is a multifactorial phenomenon, involving diverse psychosocial and biological determinants. Data from the Suicide White Paper 2024 (Cabinet Office, 2024; English summary: Summary of FY2023 General Situation of Suicide in Japan) show that the annual number of suicides in Japan hovered between 20,000 and 25,000 until 1997, but surged to 32,863 in 1998—an increase of more than 8,000 from the previous year.
Figure 1. Annual Trends in Number of Suicides in Japan (1978-2023)
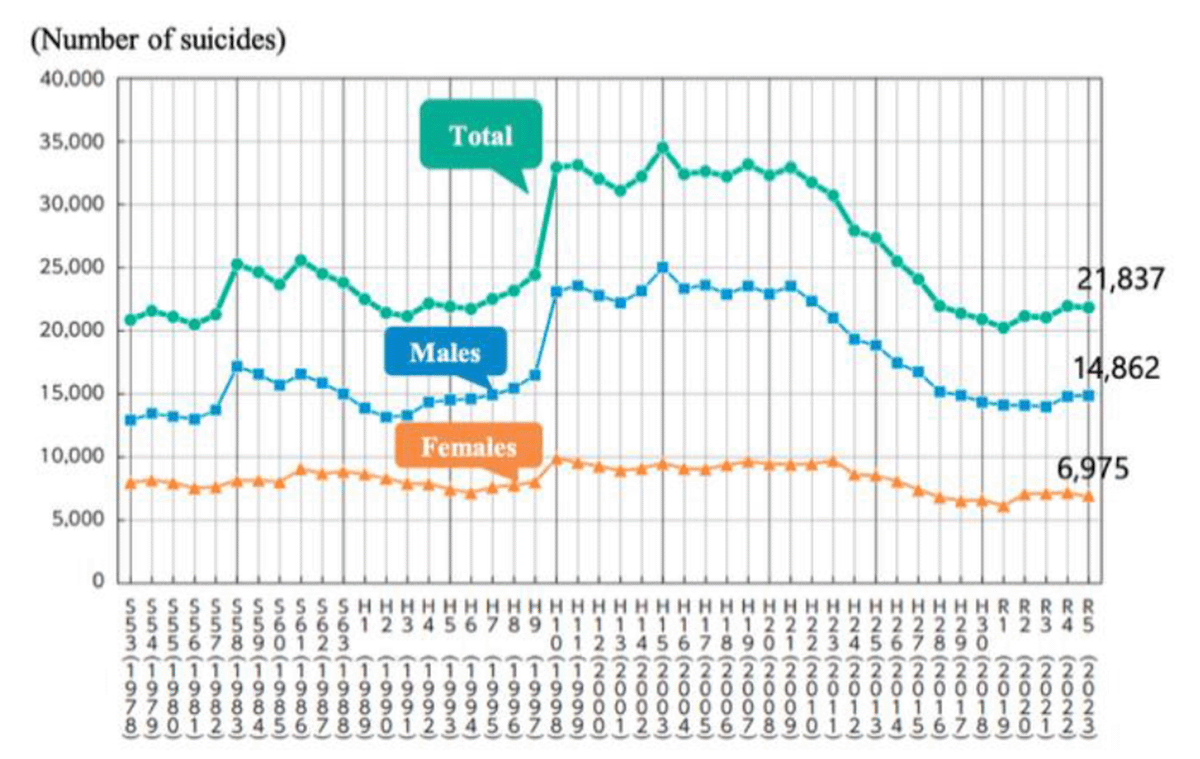
Source: Cabinet Office, Government of Japan / MHLW, White Paper on Suicide Countermeasures FY 2024
For over a decade thereafter, suicides remained above 30,000 annually, before gradually declining in the 2010s. Even so, recent figures continue to exceed 20,000 per year, underscoring suicide as an enduring social challenge.
In international comparison, Japan's suicide mortality rate (16.5 per 100,000) is the highest among G7 countries, approximately 2.7 times that of Italy (6.2), the lowest. Higher suicide rates are also noted across Nordic countries as well as in parts of East and Southeast Asia, including Japan, suggesting regional cultural and structural influences (Cabinet Office/MHLW 2024).
As National Police Agency statistics indicate, background factors include health problems, economic and livelihood distress, family issues, work-related stress, interpersonal difficulties, and school-related problems. Psychologically, conditions such as depression and adjustment disorders are significant risks; suicide is often described as "death at the end of being cornered." Before reaching the point of suicide, individuals experience severe suffering and entrapment long before death occurs.
Mental health factors include depression, schizophrenia, personality disorders, and substance dependence. When individuals are unable to access appropriate treatment, these conditions can deepen isolation, despair, and suicidal ideation.
Socioeconomic hardships such as unemployment, bankruptcy, or debt; the breakdown of interpersonal relationships; and bullying in schools also cast a heavy shadow—contexts often impossible to overcome by individual effort alone. Thus, suicide (jisatsu/jishi) should not be understood solely as an issue of individual psychology. It must be examined in a broader frame, encompassing social structures, the adequacy of support systems, and connections with communities.
3. Risk Factors Leading to Suicide (jisatsu/jishi) and Their Hierarchical Organization
The background of suicide (jisatsu/jishi) consists of diverse and interrelated factors that can be organized into three layers of individual risk. These layers operate in a continuous and overlapping manner, together contributing to the likelihood of suicidal behavior (Turecki & Brent, 2016):
- Distal / Predisposing Factors: Genetic vulnerability, adverse childhood experiences, personality traits, family history, and chronic medical conditions that form long-term, foundational risks.
- Developmental / Mediating Factors: Coping capacity, social skills, identity formation, developmental influences, and the onset of psychiatric disorders such as depression, bipolar disorder, or schizophrenia.
- Proximal / Precipitating Factors: Immediate stressors such as bereavement, job loss, or relationship breakdown, along with acute psychological pain, hopelessness, or heightened impulsivity—factors that can trigger the transition to suicidal behavior.
From this perspective, suicide prevention strategies should not attempt to address all factors uniformly. Instead, they require realistic and strategic prioritization. Distal and developmental issues, for example, may be more appropriately addressed not solely within the framework of suicide prevention, but through broader domains such as education, family support, and community healthcare.
By contrast, the direct prevention of suicide requires interventions targeted at individuals already trapped in the conviction that "there is no alternative but death." Two core areas are especially critical (Turecki et al., 2019):
- Evaluation and Prevention of Suicide-Related Behavior: Mental health support, responsive care for suicidal ideation, restriction of access to lethal means (e.g., pesticide and medication control, physical barriers at high-risk sites such as buildings or bridges), responsible media reporting practices, and the establishment of clear guidelines.
- Risk Assessment: Early identification of individuals at risk and the development of systems for timely intervention.
Focusing resources on these domains is essential to maximize the effectiveness of suicide prevention.
4. Institutional Evolution and Effectiveness of Suicide (jisatsu/jishi) Countermeasures in Japan
Japan's suicide countermeasures have progressively developed institutional frameworks since the early 2000s, with stronger support for local implementation systems. A major turning point came with the enactment of the Basic Act on Suicide Countermeasures (2006) and the subsequent General Principles of Suicide Countermeasures Policy (2007), which institutionalized a comprehensive approach involving collaboration among national government, local municipalities, and civil society. Later measures introduced targeted interventions for high-risk groups, the Gatekeeper program, and more recently, outreach using social media to support younger cohorts. Yet challenges remain, including uneven service delivery, disparities in implementation capacity, and insufficient integration with digital technologies.
The evolution of Japan's suicide prevention measures can be summarized under three perspectives:
(1) Depression Countermeasures
Although experts had long recognized the seriousness of suicide (jisatsu/jishi), it was not articulated as a national policy goal until the early 2000s. In March 2000, the government launched Health Japan 21, aimed at reducing premature mortality, extending healthy life expectancy, and improving quality of life. Within its analysis, suicide was identified alongside cancer and accidents as a leading cause of early death, measured using potential years of life lost (PYLLSR). Disability-adjusted life years (DALY) were also used to highlight suicide's broader impact. Within its indicators, suicide was listed alongside cancer, stroke, and heart disease as a major target for reduction. Suicide was treated as a health issue, and within mental illness, depression was identified as a priority risk state to address, with the goal of "establishing appropriate treatment systems for depression and related conditions to reduce suicides." The measures outlined at that time included: (i) strategies to maintain mental health, such as stress and sleep management, and (ii) responses to mental illness, including dissemination of knowledge about suicide risk factors, warning signs, and appropriate responses; expanding public understanding of the symptoms of depression and effective treatments; and strengthening collaboration among primary care physicians, psychiatrists, public health nurses, and teachers. As such, the initial suicide countermeasures were presented largely as mental health measures, in particular depression countermeasures, meaning that suicide was addressed in the same way as other health problems. However, the related Health Promotion Act only mentioned lifestyle factors such as diet, exercise, rest, alcohol, smoking, and oral health, and did not contain direct reference to suicide.
(2) Revision of the Basic Act — Clarifying Social Responsibility to Protect Children
The 2025 revision of the Basic Act on Suicide Countermeasures was a landmark, explicitly prioritizing child and youth suicide prevention. This revision emphasized the fact that suicide is the leading cause of death among teenagers in Japan and created a strengthened legal framework to ensure that "society as a whole protects children's lives." Key elements included:
- Explicitly stating the principle that children should be able to "create a society where children can grow up healthy and live,” with responsibility shared by families, schools, and communities.
- Addressing digital-era risks such as online suicide-related information and exploring the use of AI for prevention.
- Clarifying responsibilities of the Prime Minister, Ministers of Education and Health, and schools themselves, legally obligating schools to safeguard mental health and cooperate in suicide prevention.
- Strengthening implementation through school health checks, mental health education, professional training for healthcare workers, information-sharing systems for students in need of support, and continuous support for attempters and bereaved families.
However, several challenges remain. First, it is uncertain whether the philosophy of the revised law will fully penetrate practice and translate into effective support, given that schools and welfare settings are already facing staff and budget shortages. Second, responses in the digital domain, including social media and AI, are difficult not only from a technical standpoint but also in terms of ethical and legal coordination, requiring continued institutional design. Third, systems to reflect children's own voices and needs in policy remain insufficient, and a stronger support system based on the perspectives of those directly affected is needed. Going forward, it will be essential to carefully monitor the implementation of the revised law, strengthen interagency collaboration and human resource support, and ensure that countermeasures take root in practice. To build a society where no child is left isolated, what is required is not only legal structures but also the maturity of local communities grounded in empathy and understanding.
(3) Suicide Prevention and Support for the Bereaved
The 2006 Basic Act and the subsequent General Principles marked a shift toward combining targeted support for high-risk individuals with preventive approaches at the societal level. Explicit mention was made of support for the bereaved by suicide, including peer groups, specialized counseling, and awareness-raising in schools and workplaces. This policy shift between 2005 and 2007 broadened the lens from an individual, mental-health-centered framework to a multi-layered societal response, embedding bereavement care as part of comprehensive prevention.
5. Implementation of Countermeasures (Interventions) and Future Prospects
In implementing suicide (jisatsu/jishi) countermeasures, decisions cannot be based on scientific evidence alone. In public policy and public health practice, factors such as cost-effectiveness, social significance, community needs, and even public opinion or political leadership exert strong influence on decision-making. Particularly for issues suspected to have a strong relationship with suicide, there are arguments that flexible action should be considered—even where scientific validation is insufficient—if some empirical effect is reasonably expected. At the same time, distinguishing between interventions grounded primarily in experiential practice and those supported by statistical and empirical validation remains difficult. Allocating resources under such uncertainty is therefore highly complex. To guide the process, a phased approach to social implementation is essential, consisting of five steps:
- Understanding the situation: Conduct research to grasp the actual conditions and background factors related to suicide (jisatsu/jishi).
- Developing and validating interventions: Design interventions tailored to actual conditions and rigorously evaluate their effectiveness.
- Strategic design for social implementation: Formulate strategies to scale up and disseminate interventions that demonstrate effectiveness.
- Implementation and monitoring: Carry out interventions while continuously monitoring outcomes and making iterative improvements.
- Securing sustainability: Establish institutional and financial frameworks to ensure that support systems are durable over the long term.
However, the interpretation of scientific strength and intervention effectiveness varies across stakeholders. Traditional practices with limited scientific backing often coexist with pragmatic approaches emphasizing perceived or experiential benefits, complicating decision-making. Moreover, suicide (jisatsu/jishi) prevention spans highly diverse target groups with different backgrounds. Questions of which risk group to prioritize, at what timing, and with which method, often divide expert and public opinion alike.
For this reason, when interventions with limited evidence are advanced, it is critical to pair implementation and monitoring with parallel research that rigorously examines their impact. At the same time, caution is warranted against overextending the label of "suicide prevention" to broad social reforms or unrelated policy domains. Such overextension risks dispersing and diluting resources that are urgently needed for direct support to high-risk groups.
6. Conclusion — Future Prospects and Responsibilities Grounded in Empathy
This report has reviewed the current state of suicide in Japan, the trajectory of institutional responses, the challenges of intervention implementation, and perspectives required for the future. Suicide must not be reduced to an individual problem; it is a question about the very structure of society. Continuous evaluation, dialogue, and approaches rooted in empathy are essential keys to illuminating the future.
In the years ahead, suicide prevention will be tested by how well Japan can balance the accumulation of scientific evidence with the scale of the problem and the demands of society. Building this balance requires synthesizing knowledge about which interventions are appropriate, at what stage, and for which issues, while also ensuring that the public as a whole recognizes the gravity of the problem and engages in dialogue and cooperative action across different positions.
Above all, constructing support systems that leave no one behind is indispensable—especially for those who find it difficult to voice their needs, including young people, the elderly, sexual minorities, foreign workers, and the bereaved by suicide. How the voices and experiences of the bereaved are incorporated into policy formation will be a core challenge for comprehensive prevention going forward, and this will be explored in depth in the next report of this series. Moreover, new issues of the digital age, including social media and AI technologies, are closely connected to the suicide challenges faced by younger generations and will also be addressed in future reports.
Thus, the way forward for suicide prevention lies in balancing the twin wheels of scientific evidence and societal demand, and in embracing a collective "responsibility grounded in empathy." Building on the macro- and policy-level perspectives set out in this report, subsequent installments will deepen the discussion on terminology, the suffering of the bereaved, the challenges facing young people, and the evolving role of scientific evidence.
For those who are struggling
You do not have to carry painful feelings on your own. The Ministry of Health, Labour and Welfare provides information on consultation services where trained counselors offer support in confidence. These services are available both through telephone helplines and SNS- or chat-based consultation services, allowing people to seek help in a way that feels accessible to them.
Ministry of Health, Labour and Welfare - How to Seek Help / Helplines ("Mamorou yo Kokoro")
Reviewed by Masatoshi Inagaki, Ph.D., Professor, Department of Psychiatry, Faculty of Medicine, Shimane University.
[References]
- Cabinet Office, Government of Japan. (2024). White paper on suicide countermeasures, FY2024: Summary of FY2023 general situation of suicide in Japan. https://www.mhlw.go.jp/content/001464705.pdf
- Ministry of Health, Labour and Welfare. (2012). Health Japan 21 (the second term). https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/kenkounippon21.html
- Ministry of Health, Labour and Welfare. (2012). Ministerial Notification No. 430 of the Ministry of Health, Labour and Welfare. https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000047330.pdf
- Ministry of Justice. (2025). Basic Act on Suicide Countermeasures (Act No. 85 of 2006; revised 2025). https://laws.e-gov.go.jp/law/418AC0100000085
- National Police Agency. (2023). Situation of suicide in 2023. https://www.npa.go.jp/safetylife/seianki/jisatsu/R05/R05_jisatuno_joukyou.pdf
- Turecki, G., Brent, D. A., Gunnell, D., O'Connor, R. C., Oquendo, M. A., Pirkis, J., & Stanley, B. H. (2019). Suicide and suicide risk. Nature Reviews Disease Primers, 5(1), 74. https://doi.org/10.1038/s41572-019-0121-0
- Turecki, G., & Brent, D. A. (2016). Suicide and suicidal behaviour. The Lancet, 387(10024), 1227-1239. https://doi.org/10.1016/S0140-6736(15)00234-2
- World Health Organization. (2023). Recommendations for reporting on suicide for the media - A guide for media professionals (Japanese edition). https://iris.who.int/bitstream/handle/10665/372998/9789290619797-jpn.pdf
Original in Japanese:
https://www.dlri.co.jp/report/ld/512312.html
[Version Note]
First published on Sep 2, 2025.
Updated March 16, 2026: Minor revisions made to align with Part 2 of the Suicide Prevention series.
Disclaimer:
This report has been prepared for general information purposes only and is not intended to solicit investment. It is based on information that, at the time of preparation, was deemed credible by Daiichi Life Research Institute, but it accepts no responsibility for its accuracy or completeness.